Table of content
- What Are the Main Types of Insulin & How Are They Different?
- Rapid-Acting vs. Short-Acting: Why the Difference Matters
- What Is Long-Acting Insulin and Who Needs It?
- Can Different Insulin Types Be Mixed Together Safely?
- The Practical Comparison of Injections vs. Insulin Pumps
- Conclusion
- Frequently Asked Questions
Starting insulin is overwhelming. You get a prescription, a needle, and maybe a 10-minute explanation, then you are on your own. Blood sugar spikes after lunch. You wake up at 3 am too high or too low. And you have no idea why.
Most insulin guides list types and timing. But they never tell you what is secretly affecting your insulin every day or why the same dose that worked last week suddenly does not.
This guide covers it all. The five insulin types, a clear onset and peak reference, safe mixing rules, and five hidden factors most guides skip. By the end, you will understand your insulin better than most patients do after years on it.
What Are the Main Types of Insulin & How Are They Different?
Insulin is classified by three things:
- Onset: When it starts working.
- Peak: When it is strongest.
- Duration: How long it lasts.
According to the American Diabetes Association, there are five main categories used in diabetes treatment today:
- Rapid-acting insulin: Starts in 10-15 minutes, used for meal coverage.
- Short-acting (regular) insulin: Starts in 30-60 minutes, also taken before meals.
- Intermediate-acting (NPH) insulin: Starts in 1-4 hours, lasts 12-18 hours.
- Long-acting (basal) insulin: Starts in 1-2 hours, lasts 24 hours with no strong peak.
- Pre-mixed insulin: Combines two types in one injection for simplified dosing.
Each type has a specific job. Most people with Type 1 diabetes and many with Type 2 diabetes need more than one type to stay in range throughout the day.
Rapid-Acting vs. Short-Acting: Why the Difference Matters
Both types cover meal-related blood sugar rises, but their timing gap trips a lot of people up. Getting this wrong is one of the most common reasons blood sugar runs high after eating.
- Rapid-acting insulin (Lispro, Aspart, Glulisine) starts working in about 10-15 minutes. Inject it right before you eat. It peaks in 1-2 hours and clears your system in 3-5 hours. It works faster and fits modern lifestyles better.
- Short-acting regular insulin takes 30-60 minutes to kick in. You need to inject it half an hour before meals.
Very rapid-acting insulins like Fiasp and Lyumjev begin working in as little as 2-5 minutes, designed for people who struggle with pre-meal timing or prefer to dose during or right after a meal.
People using the Omnipod 5 tubeless pump remove this timing stress entirely. It reads CGM data continuously and adjusts rapid-acting insulin delivery automatically throughout the day.
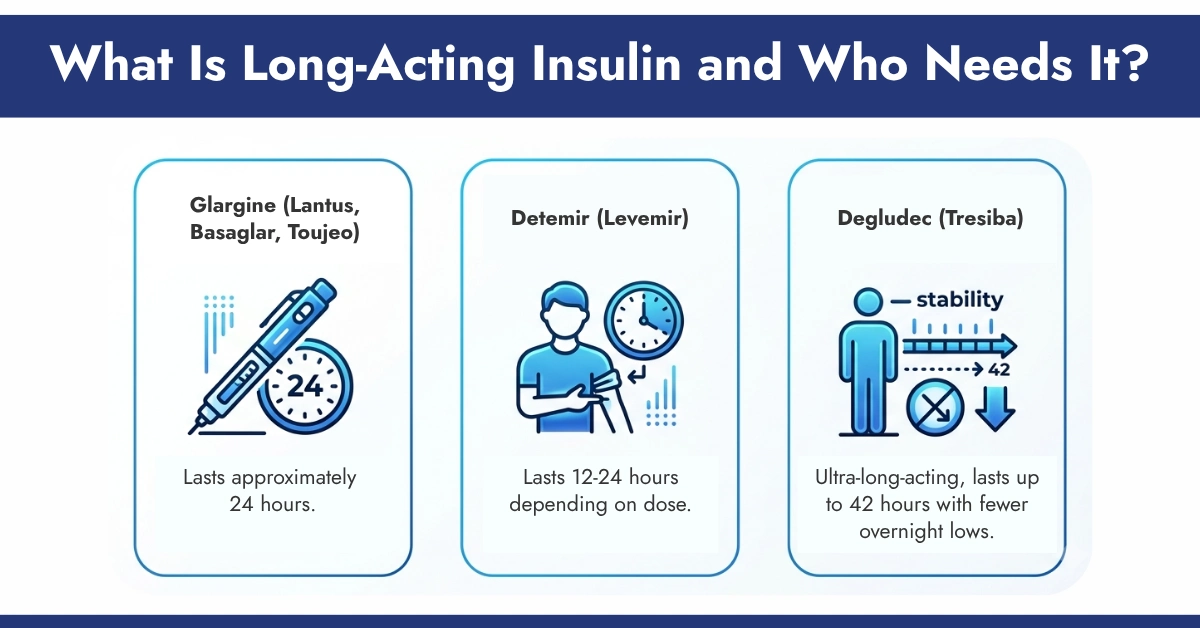
What Is Long-Acting Insulin and Who Needs It?
Long-acting insulin, also called basal insulin, does not spike your system. It releases slowly and steadily all day and night, keeping blood sugar stable between meals, during fasting, and while you sleep.
Common options include:
Glargine (Lantus, Basaglar, Toujeo): Lasts approximately 24 hours.
Detemir (Levemir): Lasts 12-24 hours depending on dose.
Degludec (Tresiba): Ultra-long-acting, lasts up to 42 hours with fewer overnight lows.
Who needs it?
- People with Type 1 diabetes are always, without exception.
- People with Type 2 diabetes whose fasting blood sugar stays high despite oral medications.
- Anyone waking up with consistently elevated morning glucose levels.
Without basal insulin, blood sugar climbs even when you don’t eat. The liver keeps releasing glucose with nothing to balance it.
What Is Basal-Bolus Therapy and Who Benefits Most?
Basal-bolus therapy is the gold standard in insulin management. It combines:
- Basal insulin: Injected once or twice daily for steady, all-day background coverage
- Bolus insulin: Rapid-acting, taken before each meal to handle carbohydrates
Together, they mimic how a healthy pancreas works naturally, a slow trickle all day (basal) and a bigger burst at meals (bolus).
The challenge is that it requires 4 or more injections daily and careful calculations. This is why many people eventually move to insulin pumps. The Tandem t:slim X2 delivers both basal and bolus insulin and integrates directly with CGM sensors, automatically adjusting doses based on where your glucose is trending, not just where it sits right now.
Can Different Insulin Types Be Mixed Together Safely?
Mixing insulin sounds simple. It is not. Some combinations are safe. Others reduce effectiveness or create dangerous absorption problems.
| Combination | Safe to Mix? | Keynote |
| Rapid-acting + NPH | Yes | Draw rapid-acting into the syringe first. |
| Regular (short-acting) + NPH | Yes | Standard, widely used combination. |
| Glargine (long-acting) + any | No | Different pH alters effectiveness of both. |
| Detemir or Degludec + any | No | Mixing affects absorption unpredictably. |
| Pre-mixed insulin + anything | No | Already balanced, never alter the ratio. |
Critical warning:
Long-acting glargine is a clear liquid identical in appearance to rapid-acting insulin. Accidentally injecting the wrong one has sent real patients to the ER. Always store each type separately and use clearly labeled, dedicated pens.
What Are the 5 Things That Quietly Change How Your Insulin Works?
- Injection site: Repeated use causes fat buildup → slower absorption.
- Exercise: Increases insulin sensitivity → risk of sudden lows.
- Stress & illness: Hormones raise blood sugar → need more insulin.
- Temperature: Heat speeds absorption, cold slows it.
- Dawn phenomenon: Morning hormone surge raises blood sugar.
These factors explain why the same dose behaves differently every day
The Medtronic insulin pump system addresses the Dawn Phenomenon directly; its Smart Guard technology uses overnight CGM readings to automatically adjust basal delivery before the morning rise even begins. If you are confused about the Dawn Phenomenon vs the Somogyi Effect, please check our article that gives you a complete insight into it.
The Practical Comparison of Injections vs. Insulin Pumps
Both methods work well, but they fit very different lifestyles.
Injections (pens or syringes):
- Simple, low-cost, no device to wear or charge.
- Require multiple daily injections for basal-bolus therapy.
- Great starting point for newly diagnosed patients.
Insulin pumps:
- Deliver continuous basal insulin automatically.
- Allow precise bolus doses at the press of a button.
- Work best when paired with a CGM for real-time adjustments.
Conclusion
Understanding insulin types is more than memorizing numbers on a chart. It is knowing why your insulin works, and why it sometimes does not. The five hidden factors, safe mixing rules, and the Dawn Phenomenon are what actually make a difference in daily life.
At CGM Monitors, we make insulin management easier, with trusted CGM devices, insurance support, free delivery, and monthly refills delivered to your door.
Disclaimer:
This content is only to help you understand insulin types, diabetes management, and CGM-based monitoring systems simply. It is made for learning and general information only, not medical guidance. Always consult your doctor before starting, stopping, or adjusting any insulin, medication, or diabetes-related therapy. CGM Monitors does not diagnose, treat, or replace medical care. Some images used in this article are AI-generated and are included for illustration and visual understanding purposes only.
Frequently Asked Questions
Is once-weekly insulin available yet?
Weekly basal insulin is now emerging. Insulin Icodec is already approved in the European Union. Insulin Efstiora has shown results comparable to daily degludec in U.S. clinical trials. Neither is widely available in the U.S. as of April 2026, but they are a major step forward for patients who struggle with daily injections. Ask your endocrinologist about availability.
Does it matter what time of day I take long-acting insulin?
Consistency matters more than the specific hour. Bedtime works well for many people because it aligns coverage with overnight fasting. Morning works better for others. If your morning blood sugars are consistently high or low, your doctor can adjust the timing using your CGM pattern data.
Can insulin behave differently in summer vs winter?
Yes. Heat increases blood flow under the skin, speeding up insulin absorption. Cold slows it down. In hot weather, insulin may act faster than expected, raising your risk of lows. In cold weather, absorption becomes less predictable. Monitor your glucose more frequently during extreme temperature changes.
What is the 50-50 rule in basal-bolus dosing?
It is a clinical starting guideline. Your total daily insulin dose is split roughly 50% basal and 50% bolus, divided across meals. At 40 units total daily, that means 20 units of long-acting insulin and about 7 units of rapid-acting insulin before each of three meals. This is a starting point only; your doctor will adjust it based on your CGM data and individual response.



Write a comment
Your email address will not be published. All fields are required